The Health Insurance Claim form 1500 or HCFA 1500 claim form, also known as CMS 1500 claim form as well. The CMS 1500 Claim Form is the uniform or standard claim form used by a provider or supplier to bill Medicare and DMERCs (durable medical equipment regional carriers) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of claims.
The NUCC- National Uniform Claim Committee is authorized and responsible for the design and maintenance of the CMS1500 forms.
Table of Contents
Sample HCFA 1500 Claim Form-CMS 1500 Form
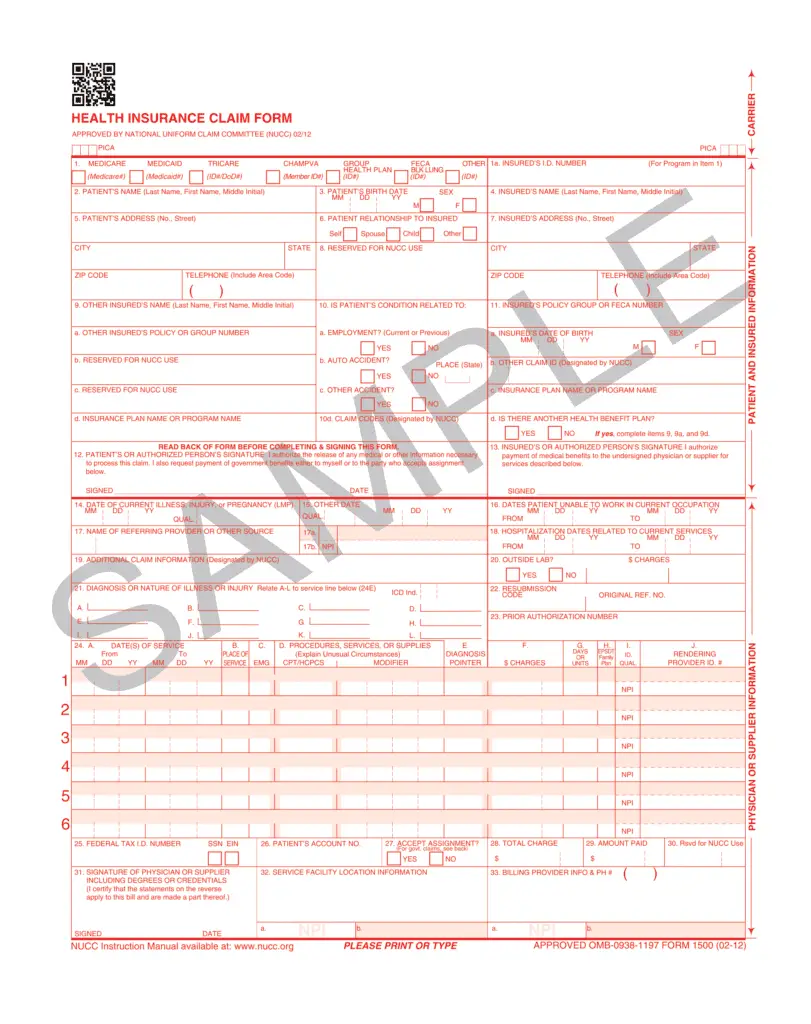
HCFA 1500 Claim Form Box Locator
| Box | Description | Required/Not Required |
|---|---|---|
| Box 1 | Type of Insurance | N |
| Box 1a | Patient’s insurance policy ID Number | Y |
| Box 2 | Patient’s Name | Y |
| Box 3 | Patients’s Date of Birth and Sex | Y |
| Box 4 | Patient’s Name (Last-First-Middle Name) | N |
| Box 5 | Patient’s Address | Y |
| Box 6 | Patient’s Relation with insured ( Self/Spouse/Child/other) | N |
| Box 7 | Insured Person Address | required when insured name updated in collumn 4 |
| Box 8 | Patient Status( Married/Single/Employed/Student/Other) | N |
| Box 9 | Other Insured’s Name | N |
| Box 9a | Other Insured’s Policy or group number | N |
| Box 9b | Other Insured’s DOB | N |
| Box 9c | Other Insured’s Employer’s name/School Name | N |
| Box 9d | Other Insured’s Plan Name | N |
| Box 10A | Patient’s condition Related to Employment | N |
| Box 10B | Patient’s condition Related to Auto Accident | As per condition |
| Box 10C | Patient’s condition Related to other Accident | As per condition |
| Box 10d | Reserve for local use | N |
| Box 11 | Insured’s Policy/ Group/ FECA Number | N |
| Box 11a | Insured’s DOB/ Sex | N |
| Box 11b | Employer Name or School Name) | N |
| Box 11c | Insurance Plan Name or programe Name | N |
| Box 11d | Is there another health benefit plan? | N |
| Box 12 | Patient’s or Authorized Person’s Signature | Y |
| Box 13 | Insured’s or Authorized Person’s Signature | As per condition |
| Box 14 | Date of Current Illness, Injury, Pregnancy (LMP) | N |
| Box15 | If Patient Has Had Same or Similar Illness give 1st date | N |
| Box 16 | Dates Patient is Unable to Work in Current Occupation | N |
| Box 17 | Name of Referring Provider or Source | As per condition |
| Box 17a | Other id | N |
| Box 17b | Referring/Ordering Provider NPI | As per condition |
| Box 18 | Hospitalization Dates Related to Current Services | As per condition |
| Box 19 | Additional Claim Information (earlier reserved for local use) | N |
| Box 20 | Outside Lab Charges | N |
| Box 21 | Diagnosis or Nature of Illness or Injury (dx codes) | Y |
| Box 22 | Resubmission and/or Original Reference Number | As per condition(6 – Corrected Claim,7 – Replacement of prior claim,8 – Void/cancel of prior claim) |
| Box 23 | Prior Authorization Number | No |
| Box 24 | Shaded Area Above. Use this area for and NDC/UPN information. | As per condition |
| Box 24a | Date of Service | Y |
| Box 24b | Place of Service | Y |
| Box 24c | EMG | In emergency case enter Y otherwise N |
| Box 24d | Procedures, Services, or Supplies | CPT or HCPCS code and modifier |
| Box 24e | Diagnosis Pointer | Y |
| Box 24f | Charges or Billed Amount | Y |
| Box 24g | Days or Units Billed | Y |
| Box 24h | EPSDT/Family Plan | N |
| Box 24i | ID Qualifier | N |
| Box 24j | Rendering Provider ID # (NPI) | As per condition |
| Box 25 | Federal Tax ID or SSN | Y |
| Box 26 | Patient’s Account Number | N |
| Box 27 | Accept Assignment | As per condition. Enter an X in the correct box noting if assignment is accepted |
| Box 28 | Total Charge | y |
| Box 29 | Amount Paid | As per condition |
| Box 30 | Reserved for NUCC Use (earlier Balance Due) | N |
| Box 31 | Signature of Physician or Supplier Including Degrees or Credentials | Y |
| Box 32 | Service Facility Location | As per condition |
| Box 32a | Service Facility NPI | N |
| Box 32b | Service Facility Other ID Number | N |
| Box 33 | Billing Provider Info and Phone Number | Y |
| Box 33a | Billing Provider NPI | Y |
| Box 33b | Billing Provider Other ID Number | N |
The CMS 1500 form (HCFA-1500) is used to submit charges covered under Medicare Part B or for professional billing claims.
CMS1500 (PDF)- HCFA 1500 Claim Form Download PDF
Image source and Information Reference– www.cms.gov
Related Article:
- How to Overcome Revenue Cycle Management Challenges in 2026?
- Medicare Health Insurance Complete Guide
- Health Insurance Claim Form – Sample HCFA 1500 Claim Form
- Timely Filing Limit in Medical Billing (2026)
- 5 Ways to Improve Patient Retention (2026)
Insurance Claim Address (A to Z)
Workers Compensation Insurance List and Phone Number
Molina Healthcare Phone Number| Molina Claim Address

The author and contributor of this blog "NSingh" is working in Medical Billing and Coding since 2010. He is MBA in marketing and Having vaste experience in different scopes of Medical Billing and Coding as AR-Follow-up, Payment Posting, Charge posting, Coding, etc.